 Tele-consultation
Tele-consultation
 Make an appointment
Make an appointment
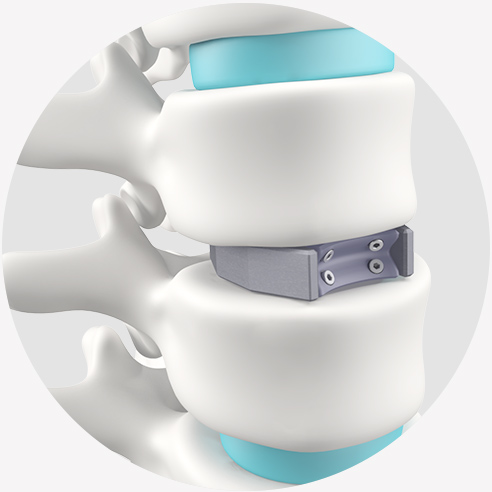

Why operate through the abdomen
The disc is in the front part of the spine, while the nerves and spinal cord pass through a canal at the back of the spine. By accessing the disc via the abdomen, the ALIF cage can be placed without disturbing the nerve roots; so, there is less risk of damaging the spinal nerves than with the more traditional techniques of approaching the spine through the back (posterior approach).
 4 to 8 cm
4 to 8 cm
Abdominal scar, above the pubis
 45 min.
45 min.
Duration of surgery
 1 to 3 days
1 to 3 days
Average length of hospital stay
 6 weeks
6 weeks
Restraint with a custom-made removable plastic brace
 6 to 12 months
6 to 12 months
Average recovery time
 3 months
3 months
Minimum duration of absence from work
 6 weeks
6 weeks
Period before starting back driving
 4 to 6 months
4 to 6 months
Period before resuming sports activities
 10 days
10 days
Flying home after surgery
 1 year
1 year
Duration of evolution up to the final result of the surgery, in the absence of neurological sequelae